Potential Life In The Doctrine
In their article, Abortion: A Woman’s Private Choice,[1] Erwin Chemerinsky and Michele Goodwin seek to shore up the doctrinal basis for a woman’s constitutional right to end her pregnancy. While Chemerinsky and Goodwin are partly concerned about the status of abortion rights in the United States because of President Donald Trump’s promise prior to taking office to appoint Justices to the Supreme Court who will overturn Roe v. Wade,[2] they also maintain that some of the threat to abortion rights arises from an uncomfortable tension in the doctrine that recognizes states’ interest in potential life.[3] I agree with Chemerinsky and Goodwin that the undue burden standard, especially how it has been applied, under-protects the constitutional right to an abortion. But the existing doctrine still provides more limits on the government’s ability to enact abortion restrictions than Chemerinsky and Goodwin suggest, even where the government purports to protect potential life. The threat to abortion rights is real, but it is not just from the undue burden standard: it is from politicians who, with the help of lawyers, will continue to try and legislate abortion out of existence and drain the legal standards governing abortion of any meaning. After outlining the undue burden standard, Part I explains why the state’s interest in potential life poses a challenge to the undue burden standard. Part II outlines how the undue burden standard nonetheless limits states’ ability to restrict abortion even when they purport to vindicate an interest in potential life. Part III suggests that the challenge to abortion rights arises more from states’ willingness to baldly challenge the legal standard governing abortion restrictions than from the legal standard itself.
I. Challenges in the Doctrine
Planned Parenthood of Southeastern Pennsylvania v. Casey[4] reaffirmed Roe v. Wade’s central holding that women have the right to end their pregnancies before viability.[5] But as Chemerinsky and Goodwin explain, the decision at best uncomfortably embraced the idea that a woman’s decision to end a pregnancy is a constitutionally protected liberty. Casey replaced Roe’s trimester framework with the undue burden standard because Roe’s trimester framework purportedly did not “fulfill [the] . . . promise that the State has an interest in protecting fetal life or potential life.”[6] As Chemerinsky and Goodwin recognize, there is “an internal tension” in this part of Casey: The Court declared that the state has an interest in the very thing an abortion does away with—a “potential life.”[7]
Casey declared: “[A]n undue burden is a shorthand for . . . a state regulation” that “has the purpose or effect of placing a substantial obstacle in the path of a woman seeking an abortion.”[8] Laws with either an impermissible purpose, or an impermissible effect are invalid under that standard. Just this past term, the Supreme Court spelled out how Casey’s undue burden standard works in Whole Woman’s Health v. Hellerstedt.[9] Whole Woman’s Health explained that states must demonstrate that a restriction on abortion actually furthers a permissible purpose: Casey “requires that courts consider . . . the benefits” a law actually provides—that is, the benefits that a state can show its law provides beyond the state’s mere assertions.[10] Whole Woman’s Health then went on to say that Casey also requires courts to “weigh[] the [law’s] . . . benefits against [its] burdens.”[11]
That much seems unobjectionable. But one problem with the undue burden standard may be how the standard applies where the government purports to be expressing an interest in potential life. In those cases, how is a court to assess whether a law furthers that purpose, which Casey says is permissible, instead of the impermissible purpose of burdening a woman seeking an abortion? Where a state purports to protect women’s health, there is an independent metric that a court can use to assess whether a law furthers the state’s purpose—whether a restriction improves the health outcomes of women who obtain abortions. But what is the measure of whether a state has protected its interest in potential life? The extent to which the state reduces the number of abortions? That would make little sense because laws that substantially restrict abortions would be undue burdens because of their effects. Without another way to measure the state’s interest in potential life, the “purpose” part of the undue burden standard could collapse into the “effects” part.
Winnowing the undue burden standard down to an effects-only test is especially troubling because it may not be clear how and to what extent a measure designed to dissuade women from obtaining an abortion actually does so, at least before the restriction goes into effect.[12] Compare the restrictions that were at issue in Whole Woman’s Health, which would have required abortion providers to meet the requirements of ambulatory surgical centers, and would have required doctors performing abortions to have admitting privileges at nearby hospitals.[13] Even before the law went into effect, it was possible to assess which providers and which clinics complied with the ambulatory surgical center requirements, or the admitting privileges requirement.[14] The same is unlikely to be the case when a state enacts a measure that does too much to dissuade women from obtaining an abortion because it is hard to know, ex ante, which women might be impermissibly dissuaded from obtaining an abortion.
That difficulty is not alleviated by Whole Woman’s Health’s clarification that a restriction on abortion is facially invalid if it operates as a burden on a “large fraction” of “[women] for whom the [provision] “is an actual rather than an irrelevant restriction.”[15] Identifying the women for whom the provision is an actual restriction is the challenge because it requires judges, ex ante, to determine how a woman seeking an abortion might respond to the state expressing a preference that she choose childbirth instead.[16] And there are reasons to be skeptical of judges’ institutional competence to adopt the perspective of a woman seeking an abortion. Only 30 to 40 percent of federal appellate and trial judges are female,[17] and there are only 82 women of color serving as active federal judges.[18] Those statistics are especially troubling given that less than ten years ago, an all-male majority of the Supreme Court declared that “it seem[ed] unexceptionable to” them to “conclude some women come to regret their choice to abort,” and as a result suffer “[s]evere depression and loss of [self-]esteem.”[19] Subsequent research has proven that claim false.[20]
Finally, there is also some uncertainty about how courts can balance the state’s interest in potential life against the burdens that a restriction imposes on women. Where a state restriction purports to protect women’s health, the benefits and burdens are measured by the same unit—women’s health. But how does the state’s interest in potential life weigh against increased risks to women’s health? Gonzales v. Carhart,[21] the decision upholding the federal ban on intact dilation and evacuations (D&Es), illustrates how women’s health may get short-changed in that equation.[22] Carhart upheld the ban on intact D&Es because it furthered the government’s interest in potential life even though the American College of Obstetricians and Gynecologists, among other groups, had concluded that in all cases, intact D&Es pose fewer risks than the alternative procedure (disarticulation), and that intact D&Es especially pose fewer risks for women with particular medical conditions.[23]
II. Solutions in the Doctrine
Chemerinsky and Goodwin are prepared to throw up their hands and say that the cases “offer[] no guidance as to which laws are an undue burden and which are not.”[24] But the Court’s cases do provide some guidance for the kinds of laws that would unduly burden women’s ability to decide to end their pregnancies, even where the government purports to assert an interest in potential life. Casey, for example, suggests how the purpose part of the undue burden standard retains independent meaning in cases involving the state’s interest in potential life—if courts took Casey’s statement of that interest at its word, i.e., as an interest in potential life. If the state’s interest is in potential life, measures would be reasonably designed to further that interest only if they operated where there is potential life, i.e., before an abortion. The state’s interest in potential life does not allow states to impose various post-abortion rituals.[25]
There are also ways for judges to weigh how a restriction might have the effect of imposing a substantial obstacle on women seeking an abortion besides speculating about the number of women who might be deterred from obtaining an abortion. For example, in Whole Woman’s Health, the Court concluded that reducing the number of clinics burdened a woman’s right to obtain an abortion because it would affect “the kind of individualized attention, serious conversation, and emotional support that doctors at less taxed facilities may have offered.”[26] If “individualized attention” matters, then that would be a reason to be skeptical of state laws that post signs in public places, such as restaurants or bathrooms, announcing that the state objects to abortion.[27] And if “serious conversation” also matters, then that would be a reason to be skeptical of state laws that communicate the state’s pro-childbirth message in terms that do not reflect the solemnity of the state’s position.
Whole Woman’s Health limits states’ ability to restrict abortion in the name of potential life in other ways as well. For example, by reaffirming that the quality of care women receive matters in the “burden” part of the undue burden analysis, Whole Woman’s Health requires courts to assess the effect that any abortion restriction has on women’s health.[28] If a state bans a method of performing abortions that the state believes does not adequately respect potential life, that ban would still be invalid if it does not adequately respect women’s lives and women’s health and women’s safety. Carhart applied that kind of analysis when it upheld the ban on intact D&Es,[29] and weighed the ban’s effects on women’s health against the extent to which the ban furthered the state’s interest in potential life.[30] One might disagree, as I do, with how the Court weighed the relevant evidence. The Court appears to have waved its hands and said that while trained medical doctors had explained why intact D&Es pose fewer risks than the alternative procedure, no studies had documented that those risks had actually materialized in the alternative procedure,[31] which had “overall complication rates . . . [that] were comparable” to intact D&Es.[32] It’s not clear, however, that Carhart’s misapplication of the undue burden standard is a reason to abandon the standard, or even the doctrine’s claim that states have a legitimate interest in potential life. Carhart might be evidence that the Court isn’t great at understanding how medical risk rather than actualized harm works, but that isn’t unique to the undue burden standard, or to laws respecting an interest in potential life.
Casey also grounded the doctrinal basis for the constitutional right to an abortion in “personal dignity.”[33] Elsewhere the Court has recognized that laws imposing a stigma on individuals deprive those individuals of dignity.[34] Casey’s statement that a woman’s dignity allows her to make the decision to terminate her pregnancy could limit the ways a state is permitted to express its interest in potential life in other ways as well. For example, why can states assume that a woman who seeks an abortion does not “know that there are philosophic and social arguments”[35] for childbirth absent graphic state messaging to that effect? The state’s interest in ensuring she does could also be effectuated through rigorous sex-education programs that cover the science of childbirth, abortion, and birth control.
So, back to the tension that Chemerinsky and Goodwin see in Casey—the doctrine simultaneously embraces the idea that abortion can be a constitutional right, and the idea that the government can use some of its powers to discourage the exercise of that right. There is a way to make sense of this part of Casey that would not render the decision incapable of safeguarding a woman’s right to end her pregnancy, which is that the language from Casey does not mean that actually preventing an abortion is a permissible goal for the state to have. Were it otherwise, the restrictions at issue in Whole Woman’s Health would have been valid solely because they shuttered abortion clinics, and would have reduced the number of abortions performed in the state. But it cannot be the case that plaintiffs simultaneously prove that a restriction on abortion is constitutional when, in the words of Whole Woman’s Health, they “satisf[y] their burden” of showing that a restriction impedes access to abortion.[36]
Rather, the permissible interest that Casey has in mind is the state’s ability to “express[] a preference” against abortion—instances where some kind of government speech conveys the state’s desired message about abortion and childbirth before a woman makes her decision between the two.[37] The “substantial state interest in potential life throughout pregnancy,” allows the government to make “attempts to influence a woman’s decision,”[38] not to hinder her decision without engaging with it.[39] Were it otherwise, a plaintiff would prove that a restriction furthered a legitimate governmental interest merely by “satisfying [her] burden” of showing that the state’s chosen method of expressing respect for potential life functioned as a substantial obstacle to women seeking an abortion. To the extent that Casey spoke of an interest in dissuading a woman from terminating her pregnancy, that interest has to be understood in the terms that Casey used to describe it elsewhere—an interest in ensuring that a woman who seeks an abortion “know[s] that there are philosophic and social arguments”[40] for childbirth, and that she “contemplates” those arguments.[41] That interest is not vindicated by laws, like the one recently enacted in Ohio, that merely ban abortions after 20 weeks.[42] Those laws make it more difficult to obtain an abortion without engaging with the reasons to end a pregnancy or carry it to term.
III. Threats in the Doctrine
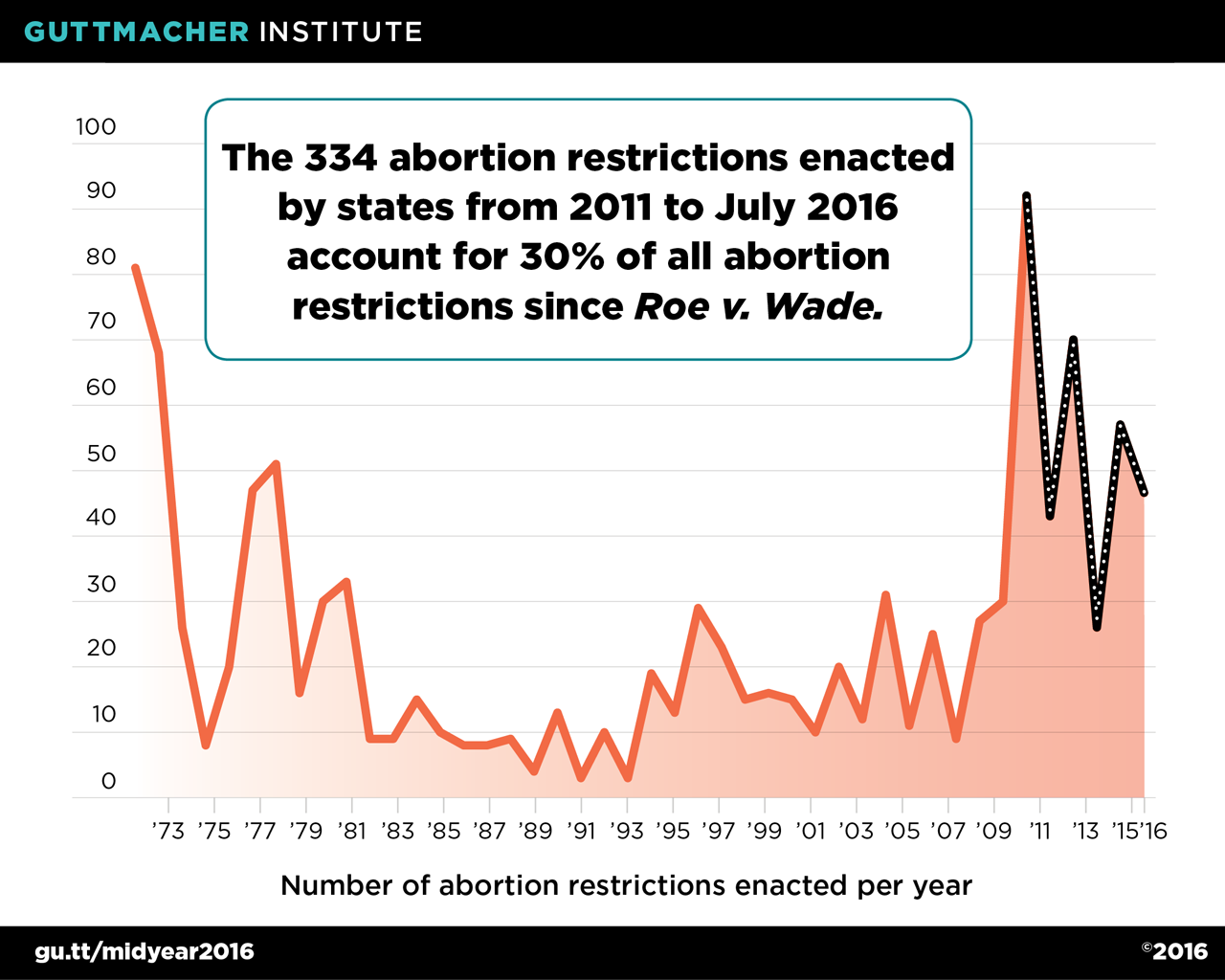
Although the current doctrine could limit a state’s ability to obstruct access to abortion under the guise of expressing an interest in potential life, states will continue to test and resist these limits, as they did in the aftermath of Carhart and as they continue to do now. In the wake of Carhart, there was a significant uptick in the number of state restrictions on abortion. The Guttmacher Institute has documented how during the 1980s and 1990s, as many as thirty abortion restrictions were enacted per year.[43] That number rose to over ninety per year soon after Carhart, and states have continued to enact abortion restrictions—the institute estimates that 30% of all abortion restrictions were enacted between 2011 and July 2016.[44] Texas was among the states to recently enact abortion restrictions, including the pair that led to the decision in Whole Woman’s Health.[45]
In Whole Woman’s Health, the Court resisted the idea that these developments were somehow attributable to Carhart, or to the undue burden standard. Carhart had simultaneously proclaimed that legislatures have “wide discretion to pass legislation in areas where there is medical and scientific uncertainty,”[46] and that courts “retain[] an independent constitutional duty to review factual findings where constitutional rights are at stake.”[47] Texas selectively relied on the former statement to argue that states do not have to show that laws restricting abortion further women’s health so long as there is “medical uncertainty” about the law’s purported health benefits.[48] The state’s understanding of Carhart, however, would have allowed states to ban abortions merely by declaring that abortions pose some risk. And in Whole Woman’s Health, the Supreme Court rejected that understanding of the undue burden standard and resolved Carhart’s apparent inconsistency.[49] As it did so, the Court notably, and pointedly, rejected the state’s understanding of the undue burden standard as an incorrect statement of Casey and the Court’s prior decisions, rather than merely rejecting the state’s view of the undue burden standard in the course of deciding between permissible readings of the Court’s prior cases.[50]
However, states committed to restricting abortion don’t treat the undue burden standard as imposing any limits on them. They didn’t do so after Carhart, and they aren’t doing so after Whole Woman’s Health. Consider Texas’s recently enacted requirement that healthcare facilities dispose of fetal tissue by burial or scattering ashes.[51] When Texas first proposed the regulations four days after the Supreme Court’s decision in Whole Woman’s Health, it justified the regulations in terms of health and safety.[52] But requiring fetal tissue to be buried or scattered cannot be justified on grounds of health and safety after Whole Woman’s Health: The state’s regulations do not explain why the existing requirements for disposing of fetal tissue do not suffice, or why fetal tissue poses unique risks relative to other kinds of biological tissue that can be disposed of in other ways.[53] Thus, when Texas adopted the final version of the regulations months later, the state added an additional justification (it is still clinging to the specious idea that the regulation furthers women’s health): Texas attempted to tie the restrictions to its purported policy of “respect for life and protecting the dignity of the unborn.”[54]
But that is nothing more than a fig leaf to cover the state’s commitment to restricting abortion. If the undue burden standard can be so easily evaded through measures that purportedly safeguard the state’s interest in potential life,[55] that would be an additional reason to jettison the current doctrine’s claim that a state does not have to be neutral between abortion and childbirth, as Chemerinsky and Goodwin recommend.[56] The undue burden standard, as the Court has explained it, provides some tools to ensure that states do not use their ability to express respect for potential life as a means to impede access to abortion. The question is whether courts will use them and will treat the legal standards governing abortion as law, or whether they will instead effectively overrule Casey and Whole Woman’s Health by giving states free rein to legislate when states purport to be vindicating an interest in potential life.[57] If that happens, Casey’s own words may be its undoing.
- .Erwin Chemerinsky & Michele Goodwin, Abortion: A Woman’s Private Choice, 95 Texas L. Rev. 1189 (2017). ↑
- .410 U.S. 113 (1973). ↑
- .See, e.g., Ariane de Vogue, Trump: Same-sex Marriage is ‘Settled,’ But Roe v. Wade Can Be Changed, CNN (Nov. 15, 2016, 7:24 AM), http://www.cnn.com/2016/11/14/politics/trump-gay-marriage-abortion-supreme-court/ [https://perma.cc/9EEP-LPHK]. ↑
- .505 U.S. 833 (1992). ↑
- .Id. at 870–71. ↑
- .Id. at 876. ↑
- .Chemerinsky & Goodwin, supra note 1, at 1220. ↑
- .Casey, 505 U.S. at 877. ↑
- .136 S. Ct. 2292 (2016). ↑
- .Id. at 2309–10. ↑
- .Id. at 2310. ↑
- .This might explain Carhart’s statement that “[i]t is a reasonable inference that a necessary effect of the regulation and the knowledge it conveys will be to encourage some women to carry the infant to full term, thus reducing the absolute number of late-term abortions.” Gonzales v. Carhart, 550 U.S. 124, 160 (2007). ↑
- .Whole Woman’s Health, 136 S. Ct. at 2300. ↑
- .Brief for Petitioners at 23–24, Whole Woman’s Health, 136 S. Ct. (No. 15-274), 2015 WL 9592289. ↑
- .Whole Woman’s Health, 136 S. Ct. at 2320 (alteration in original) (quoting Planned Parenthood of Se. Penn. v. Casey, 505 U.S. 833, 895 (1992)). ↑
- .It would be possible, ex post, to assess whether a measure placed a substantial obstacle on a woman’s path. But that would be too late for the women who were prevented from obtaining an abortion. ↑
- .Women in the Federal Judiciary: Still a Long Way to Go, National Women’s Law CENTER 1 (2016), https://nwlc.org/wp-content/uploads/2016/07/
JudgesCourtsWomeninFedJud10.13.2016.pdf [https://perma.cc/9BKM-56E4]. ↑ - .Id. ↑
- .Gonzales v. Carhart, 550 U.S. 124, 159 (2007). ↑
- .M. Antonia Biggs et al., Women’s Mental Health and Well-Being 5 Years After Receiving or Being Denied an Abortion, 74 JAMA Psychiatry 169, 177 (2017) (concluding that “there is no evidence to justify laws that require women seeking abortion to be forewarned about negative psychological responses”). ↑
- .550 U.S. 124 (2007). ↑
- .See, e.g., id. at 168 (upholding the Federal Partial Abortion Ban of 2003); Fourteenth Amendment—Due Process Clause—Undue Burden—Whole Woman’s Health v. Hellerstedt, 130 Harv. L. Rev. 397, 406 (2016) (discussing the difficulty of measuring a law’s benefits and burdens, potentially leading a court to “unofficially” defer to state law by overstating the state’s interest). ↑
- .See, e.g., Brief of the American College of Obstetricians and Gynecologists as Amicus Curiae Supporting Respondents, Carhart, 550 U.S. 124 (2006), 2006 WL 2867888, at *8–10 (arguing that intact D&Es are less risky than disarticulation, particularly for women with certain chronic conditions such as heart disease, bleeding disorders, and compromised immune systems) (hereinafter ACOG Amicus). ↑
- .Chemerinsky & Goodwin, supra note 1, at 1220. ↑
- .See infra text accompanying notes 25–29 (describing the Texas abortion restriction). ↑
- . Whole Woman’s Health v. Hellerstedt, 136 S. Ct. 2292, 2318 (2016). ↑
- .An Oklahoma legislator proposed this kind of law, but appears to have abandoned it. See Ken Miller, Oklahoma Legislator Abandons Anti-Abortion Bathroom Signs Law, Associated Press (Dec. 16, 2016, 9:51 PM), http://bigstory.ap.org/article/825ded13a0a449f3bc79b4ebe4d9f5c7/oklahoma-lawmaker-backs-anti-abortion-bathroom-signs [https://perma.cc/Y78D-B9NA]. ↑
- .See, e.g., 136 S. Ct. at 2309–10, 2318 (holding that courts must consider both the burdens a law imposes on abortion access as well as the benefits arising from those laws, and must hold that the burden is “undue” if there is little benefits and substantial obstacles created by the law). ↑
- .Carhart first explained how the federal ban on intact D&Es furthered the interest in potential life in two ways: one, by proscribing a “type of abortion” that implicates particular “ethical and moral concerns,” and two, by addressing a “lack of information . . . that is of legitimate concern to the State”—namely, that the plaintiffs’ experts had acknowledged that they did not describe to their patients what intact D&Es entail. 550 U.S. at 158–59. ↑
- .Id. at 161–63. The Court acknowledged that it was “not in the circumstances . . . plac[ing] dispositive weight on [the legislature’s] findings.” Id. at 165. ↑
- .Id. at 161–62. The reasons why intact D&Es were generally safer than disarticulation concerned the relative length and number of insertions involved in the two procedures and an unquantified risk of tissue remaining in the woman. Intact D&Es were therefore recommended for women with particular medical conditions. See ACOG Amicus, supra note 23, at *11–*20. Although the law did not allow intact D&Es where necessary for a woman’s health, the Court effectively permitted them, suggesting that “[i]f the intact D&E procedure is truly necessary . . . an injection that kills the fetus” prior to an intact D&E made the intact D&E an “alternative under the Act.” Carhart, 505 U.S. at 164. ↑
- .ACOG Amicus, supra note 23, at *18. There were, however, fewer serious complications in intact D&Es. Id. ↑
- .505 U.S. 833, 851 (1992). ↑
- .E.g., United States v. Windsor, 133 S. Ct. 2675, 2693 (2013) (stating that the history and text of DOMA demonstrate that the law interferes with the “equal dignity of same-sex” couples). ↑
- .Casey, 505 U.S. at 872. ↑
- .136 S. Ct. 2292, 2317 (2016). ↑
- .505 U.S. at 883. ↑
- .Id. at 876. Carhart underscored that the Casey interest in potential life is “an interest in ensuring . . . a choice [that] is well informed.” 550 U.S. 124, 159 (2007). ↑
- .Casey, 505 U.S. at 883. Although Carhart acknowledged that “a necessary effect” of the intact D&E ban would be “reducing the absolute number of late-term abortions,” that was not how the law furthered the state’s interest in potential life. Carhart, 550 U.S. at 160. ↑
- .Casey, 505 U.S. at 872. ↑
- .Id. at 873. ↑
- .Act of Dec. 13, 2016, Am. Sub. SB 127, 2–4 (to be codified at Ohio Rev. Code § 2919.201). ↑
- .Number of Abortion Restrictions Enacted per Year, Guttmacher Institute (2016), https://www.guttmacher.org/sites/default/files/images/071midyearstaterestrictionschart.png [https://perma.cc/F5DN-A5V7]. ↑
- .Id. ↑
- .136 S. Ct. 2292, 2300 (2016). ↑
- .550 U.S. 124, 163 (2007). ↑
- .Id. at 165. ↑
- .Brief for Respondents, at 25–26, Whole Woman’s Health v. Hellerstedt, 136 S. Ct. 2292 (2016) (No. 15-1631), 2016 WL 344496, at *25–26. ↑
- .136 S. Ct. at 2309–10. ↑
- .See id. at 2309 (“The Court of Appeals’ articulation of the relevant standard is incorrect.”); id. (“Casey, however, requires that courts consider the burdens a law imposes . . . .”); id. at 2310 (“The Court of Appeals’ approach simply does not match the standard that this Court laid out in Casey . . . .”). ↑
- .25 Tex. Admin. Code §§ 1.132(18), (33), 1.136(a)(4)(A)(v), (B)(i) (2016); 41 Tex. Reg. 9732–41 (Dec. 9, 2013). The regulations define fetal tissue as a “fetus, body parts organs or other tissues from a pregnancy,” § 1.132(28), including “products of spontaneous or induced human abortion,” § 1.136(a)(4)(A)(v), (B)(i). ↑
- .41 Tex. Reg. 4773 (July 1, 2016); see also 41 Tex. Reg. 7660 (Sept. 30, 2016) (clarifying the health and safety interest as preventing the spread of disease). ↑
- .See 41 Tex. Reg. 9709–39 (Dec. 9, 2016) (addressing public comments on the regulation by frequently referring to “prevent[ing] the spread of disease” without offering a medical reason for distinguishing fetal tissue). ↑
- .Id. at 9732. ↑
- .The Texas restrictions may still impose an undue burden by, for example, raising the costs of obtaining an abortion, or by limiting abortion providers’ ability to send fetal tissue out for medical testing. Those effects would constitute undue burdens under Whole Woman’s Health. See supra text accompanying notes 8–11. ↑
- .Chemerinsky & Goodwin, supra note 1, at 1198, 1242, 1246. ↑
- .See generally Barry Friedman, The Wages of Stealth Overruling (With Particular Attention to Miranda v. Arizona), 99 Geo. L.J. 1 (2010) (describing judicial methods that effectively overrule a decision without formally doing so). ↑
{kind=link}